Congratulations to CAI HDR students Shahrokh Abbasi-Rad and Sue Lawrence whose publications were selected as joint winners of Round 1 of the CAI 2021 HDR publication competition.
Abbasi-Rad, Shahrokh; O'Brien, Kieran; Kelly, Samuel; Vegh, Viktor; Rodell, Anders; Tesiram, Yasvir; Jin, Jin; Barth, Markus; Bollmann, Steffen; "Improving FLAIR SAR efficiency at 7T by adaptive tailoring of adiabatic pulse power through deep learning B 1 + estimation." Magnetic Resonance in Medicine, (2021), 85(5), 2462–2476. DOI: 10.1002/mrm.28590
ABSTRACT
Purpose
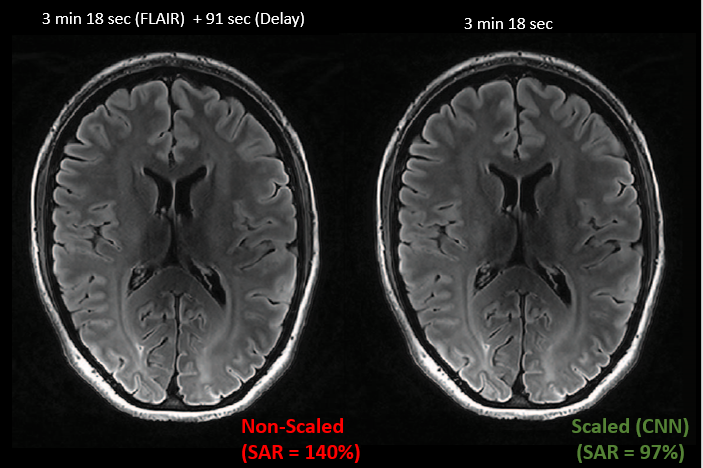
The purpose of this study is to demonstrate a method for specific absorption rate (SAR) reduction for 2D T2‐FLAIR MRI sequences at 7 T by predicting the required adiabatic radiofrequency (RF) pulse power and scaling the RF amplitude in a slice‐wise fashion.
Methods
We used a time‐resampled frequency‐offset corrected inversion (TR‐FOCI) adiabatic pulse for spin inversion in a T2‐FLAIR sequence to improve B1+ homogeneity and calculated the pulse power required for adiabaticity slice‐by‐slice to minimize the SAR. Drawing on the implicit B1+ inhomogeneity in a standard localizer scan, we acquired 3D AutoAlign localizers and SA2RAGE B1+ maps in 28 volunteers. Then, we trained a convolutional neural network (CNN) to estimate the B1+ profile from the localizers and calculated pulse scale factors for each slice. We assessed the predicted B1+ profiles and the effect of scaled pulse amplitudes on the FLAIR inversion efficiency in oblique transverse, sagittal, and coronal orientations.
Results
The predicted B1+ amplitude maps matched the measured ones with a mean difference of 9.5% across all slices and participants. The slice‐by‐slice scaling of the TR‐FOCI inversion pulse was most effective in oblique transverse orientation and resulted in a 1 min and 30 s reduction in SAR induced delay time while delivering identical image quality.
Conclusion
We propose a SAR reduction technique based on the estimation of B1+ profiles from standard localizer scans using a CNN and show that scaling the inversion pulse power slice‐by‐slice for FLAIR sequences at 7T reduces SAR and scan time without compromising image quality.
Lawrence, Sue; Malacova, Eva; Reutens, David; Sturgess, David J.; "Increased maternal body mass index is associated with prolonged anaesthetic and surgical times for caesarean delivery but is partially offset by clinician seniority and established epidural analgesia." Australian & New Zealand Journal of Obstetrics & Gynaecology. (2020) DOI: 10.1111/ajo.13277
ABSTRACT
Background
Obesity is associated with higher surgical and anaesthetic morbidity and difficulties.
Aims
We aimed to investigate associations between maternal body mass index (BMI) and the in-theatre time taken to produce an anaesthetised state or to perform surgery for caesarean delivery.
Materials and Methods
Using the Strengthening the Reporting of Observational Studies in Epidemiology guidelines, we identified all women who underwent caesarean section at a single institution (2009–2015). The prospectively collected data arising from antenatal and peripartum care were analysed. Generalised linear regression was used to examine associations between maternal BMI and the time taken to anaesthetise the mother and the duration of surgery.
Results
Of a total of 24 761 caesarean deliveries, 5607 (22.7%) women were obese at antenatal registration. In-theatre anaesthetic preparation (18 vs 32 min, P < 0.001) and surgical duration (38 vs 52 min, P < 0.001) were longer in women with BMI ≥50 kg/m2 (BMI-50) than those with normal BMI (BMI-N). This difference remained significant after controlling for antenatal, intra-operative and immediate postoperative variables. Modifiable variables were identified that may mitigate the effects of severe obesity. Senior obstetric and anaesthetic care were both independently associated with a significant reduction in mean in-theatre anaesthetic preparation time and surgical duration, by 11 and three minutes respectively (P < 0.001), while epidural top-up significantly lessened mean anaesthetic in-theatre preparation duration by seven minutes (P < 0.001).
Conclusions
Obese women had greater anaesthesia and surgery time, but the effect may potentially be mitigated by provision of care by experienced staff and prior establishment of epidural analgesia.


